
As I do from time to time, I held ’round-the clock meetings for employees on May 6. Naturally, a lot of the discussion focused on the impact of the federal health care reform legislation as it affects hospitals, as well as on the status of Community General Hospital's merger discussions with Crouse Hospital.
Health care reform legislation
I summarized the effects of the health care reform legislation – admittedly, at a very high level – on consumers, hospitals, and other organizations. For consumers, health care coverage will become more available, and an estimated 30 million individuals could be added to insurance rolls. Individuals will not be excluded from purchasing health insurance because of pre-existing health conditions, nor will there be any lifetime caps on what insurance pays for care and treatment. Adult children, up to the age of 26, will be able to have coverage under their parents’ insurance plans. This information has been generally well-covered in the news media.
I also talked about the impact of health care reform legislation on hospitals, specifically about the $196 billion reduction in Medicare and Medicaid payments to hospitals over the next ten years. There will be new taxes on medical devices and on brand-name pharmaceuticals ($31 billion over ten years), as well as the new taxes on health insurance coverage itself ($57 billion during the period). These are examples of increased costs hospitals will have to pay for the goods and services they buy.
The hospital association has translated the $196 billion nationwide reduction into the impact on each hospital in New York State. Because of the new legislation, the four hospitals in Syracuse, NY, will receive $424 million less from Medicare and Medicaid over ten years. These are huge numbers, and they are hard to imagine in the current context.
 These reductions in revenue are expected to be offset to some extent by revenue from individuals who will have health coverage, thanks to the legislation. It is very unlikely, however, that the revenue from the newly insured will come close to offsetting the reduced hospital payments that are forecast.
These reductions in revenue are expected to be offset to some extent by revenue from individuals who will have health coverage, thanks to the legislation. It is very unlikely, however, that the revenue from the newly insured will come close to offsetting the reduced hospital payments that are forecast.Overall the health care reform law will be a transformative force affecting the way health care is provided in our society.
Our merger talks
In this context I discussed the merger talks currently underway between Community General and Crouse Hospitals. I compared the forces acting on Community (such as, higher state taxes, the needs of physicians and medical groups, and pension costs) with some of the forces affecting Central New York generally (such as, flat population growth, an aging population, and Medicaid cutbacks). Recognizing these forces and anticipating the impact of federal health reform legislation, last January Community and Crouse entered an agreement to plan a merger, if feasible.
Moody’s, the financial analysis company, recently predicted that, as a result of federal legislation, non-for-profit hospitals will find it more difficult to borrow funds and that more hospitals will look for opportunities to consolidate.
Community and Crouse are, in fact, considering the advantages of creating a larger hospital that operates two campuses. The advantages could include the better ability to work with physicians, potentially better access to capital, more efficiency, and the ability to avoid duplicate investments. In interviews with consultants earlier this year, physicians from both hospitals suggested various ideas, and the consultants have been considering these. The consultants are getting close to a recommendation for both hospitals to consider.
Assuming both hospital boards adopt a structure recommended by the consultants, there will still be a number of steps remaining before the merger process is done. These include implementation planning with clinicians, filing a Hart Scott Rodino document with the Federal Trade Commission, and preparing a Certificate of Need (CON) application for New York State. In addition, both hospitals would have to complete “due diligence,” a process in which each hospital examines the other’s business in detail, considering such things as financial performance, business contracts, tax issues, pension obligations, property ownership, etc. The time frame for these activities could be another year or so.
Our financial performance
I also reviewed Community's financial performance through the first quarter of 2010.
I was pleased to report that through March, Community is operating in the black and on-budget (see the chart below). This is significantly better financial performance than we experienced in 2009 in the first quarter. 
Patient satisfaction
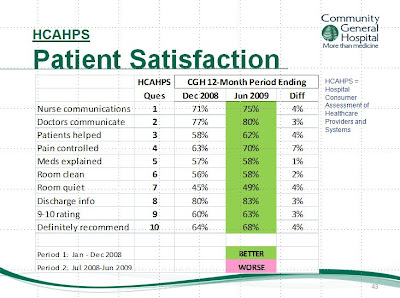
I discussed patient satisfaction and showed how Community's most recent HCAHPS scores – as self-reported by Medicare patients – have improved in every category.
The HCAHPS survey measures the percentage of Medicare patients who report that nurses and doctors “always” communicate well, that their pain is “always” well-controlled, and that their rooms are “always” well-cleaned. Community does well in comparison with other Syracuse hospitals – we have the highest scores in three of ten categories and the second highest scores in another five categories. And . . . Community's HCAHPS scores improved in the most recent 12-month period (see the chart, below).
Improvements to come
I talked about improvements being made to patient rooms on several units. The sixth floor renovation (orthopedics) has been completed, and room improvements are underway on Three West. Furthermore, we have begun to update rooms on Four West and, when finished in late summer, the patients and staff from Two West will relocate to Four West to take advantage of the updated and larger rooms. Following that, we will make improvements to the GYN rooms on Two East.
The new health information exchange
Community will become the first hospital in Syracuse this year to link to the health information exchange (HIE) being developed by the Health Advancement Collaborative of Central New York (HAC-CNY).
The HIE will initially link all four Syracuse hospitals, through the Internet, with five primary care physician groups, representing several hundred physicians. By next year doctors and hospitals on this fledgling network will be able to exchange patient-specific data with the consent of the patients themselves. As more physician practices join the exchange, HAC-CNY will link to other networks through the State Health Information Network of New York (SHIN-NY). The idea is to make individual patient information readily available to any of that individual’s caregivers. Naturally, there are demanding security and patient privacy requirements for this to function.
Employees had a number of questions and suggestions during the meetings, and I appreciated the opportunity to speak with so many of you.



No comments:
Post a Comment